

Summary #
Two patients, a dog and a cat, presented with a corneal ulcer that was progressive and had been treated with medication by the referring veterinarians but did not respond to therapy. The patients were referred for diagnostics and treatment. I recommended corneal reconstruction with a CLCT graft (a corneo-limbo-conjunctival transposition graft, also known as a CCT or corneoconjunctival transposition) in each case and the treatment led to resolution of clinical signs. One of the patients was found to also have dry eye (the dog) and went on long term treatment with Optimmune.
Several points to remember that are extrapolated from several recent studies include:
- Dogs with dry eye are often middle age to younger, but they might also be young (1-3 years old), and they can present with only mild symptoms (conjunctival redness, mucus). Do a test tear reading (STT1 reading) in all dogs that present with mild symptoms even if they are young. Some dogs with mild signs can develop an acute presentation with deep corneal ulceration. (Sanchez RF et al 2007).
- Dogs with brachycephalic and spaniel conformations are predisposed to corneal ulcerative disease and have 11.18 and 3.13 times the odds for corneal ulcers compared to cross breeds. This data is based on a study with 834 dogs with corneal ulcers out of a population of 104,233 dogs. Pugs, Boxers Cavaliers, Shih-Tzus and Bulldogs in this study had the highest odds for corneal ulcers of all the breeds included. (O’Neill et al 2017).
- CLCTs have a high success rate in cats (100% success rate in the short term and 92% success or higher in the long term in cases with corneal sequestrum) but the technique may also be used with other types of corneal disease in cats. (Graham et al 2017)
- CLCTs have a high success rate in dogs with the largest study in dogs (418 eyes) showing 97% success rate and high clarity of the cornea after surgery (except in Pugs that have lower clarity than the rest due to pigmentation). (Cebrian et al 2020)
Further reading (enter the title in www.pubmed.com to read the abstract):
Sanchez RF, Innocent G, Mould J, Billson FM. Canine Keratoconjunctivitis Sicca: disease trends in a review of 229 cases. Journal of Small Animal Practice 2007; 48(4): 211-217
O’Neill DG, Lee MM, Brodbelt DC, Church DB, Sanchez RF. Corneal ulcerative disease in dogs under primary veterinary care in England: epidemiology and clinical management. Canine Genetics and Epidemiology. 2017; 4(10): 171.
Graham KL, White JD, Billson FM. Feline Corneal sequestra: outcome of corneoconjunctival transposition in 97 cats (109 eyes). Journal of Feline medicine and Surgery 2017;19(6):710-716.
Cebrian P, Escanilla N, Lowe RC, Dawson C, Sanchez RF. Corneo-limbo-conjunctival transposition to treat deep and perforating corneal ulcers in dogs: a review of 418 eyes and corneal clarity scoring of 111 eyes. Veterinary Ophthalmology 2020; 00: 1– 11 (early online view)
Specialist #
Rick F Sanchez BSciBiol, DVM, CertVOphthal, DipECVO, FHEA
EBVS accredited, European Specialist in Veterinary Ophthalmology
Patient #
- Kelly, dog, Bulldog, 1 year old female
- Mittens, cat exotic, 3 year old male
Anamnesis #
Kelly: red eyes for an undetermined period of time, small amount of mucoid discharge also in both eyes, that were treated with a topical antibiotic (CAF) until the right eye (OD) developed a central, small, but very painful corneal ulcer.
Mittens: sudden development of a corneal ulcer of unknown origin in the right eye. Treated with a topical antibiotic (CAF for a few days and later Soligental) but it did not respond to therapy and continued to deteriorate.
Medical imaging #
Kelly
1.

2.

3.

Kelly: the first image shows the findings described below. The second image shows the CLCT graft approximately 2 weeks after surgery, with a suture reaction around the microsutures. Corneal edema and lack of transparency of varying degrees are normal at that stage. The third image shows Kelly, seen from a distance. The right eye has already healed, Kelly has no redness or mucoid discharge, she is comfortable and the pupillary axis (vision axis) shows no scarring (there is good vision).
Mittens
1.

2.
3.
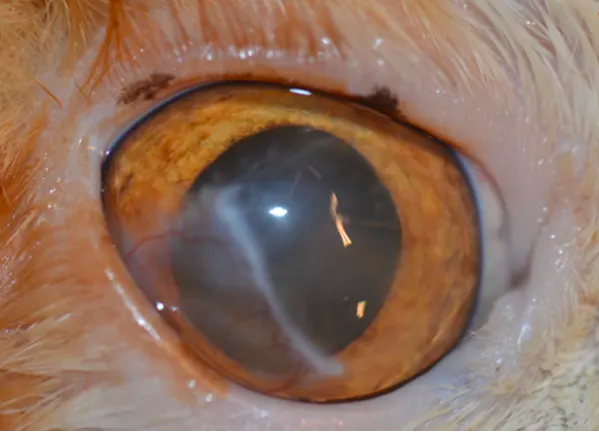
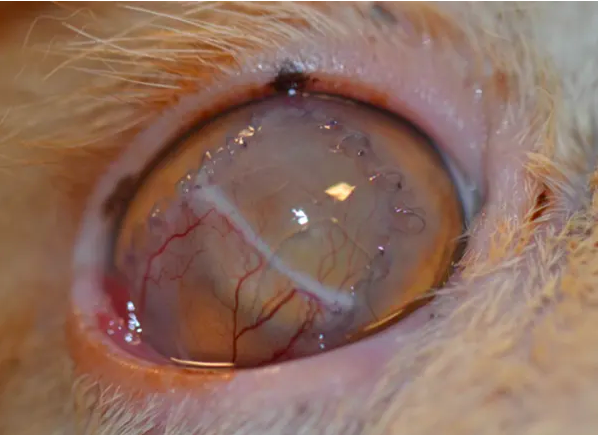
Mittens: the first image shows the findings described below. The second image shows the CLCT graft approximately 2 weeks after surgery with very little suture reaction and the expected vascularization. Note that the corneal section and the conjunctival section are very similar in level of transparency. The third image shows the eye once the sutures have completely dissolved. The corneal section of the graft is completely clear so the patient can see very well. The conjunctival section (medioventrally) is more opaque, which is expected, but still transmits light. In between is a visible white line, the limbus, which is also expected.
Findings #
The significant findings of the ophthalmic exam included the following.
Kelly: ocular pain (blepharospasm) OD only, mild to moderate conjunctival hyperemia OU (OD>OS), small amount of mucoid discharge OS only, distichiasis upper and lower eyelid OU, corneal edema OD with a centrally located small descemetocele (a deep, cratered ulcer, with a clear center that did not stain with fluorescein). STT1 readings: 16 mm/min OD (painful eye) and 10mm/min OS (ref. ≥15mm/min in the absence of clinical signs consistent with dry eye and/or pain).
Mittens: ocular pain (bepharospasm), moderate to marked conjunctival hyeremia, large and deep (75%) corneal ulcer of unknown origin OD affecting the central cornea and accompanied by stromal melting (i.e. irregular corneal surface and mucus-like surface), corneal edema and vascularization.
Diagnose #
Kelly: bilateral distichiasis, primary dry eye (KCS, bilateral) with an acute ulcerative presentation (OD) that has deteriorated into a descemetocele.
Mittens: deep, melting corneal ulcer of unknown origin (and affected by the ‘brachycephalic factor’).
Treatment & therapy #
Corneal reconstruction with CLCT in each case, followed by medical therapy consisting on a topical antibiotic (chloramphenicol drops, combined with gentamicin drops in the cat) until healing of the graft, oral NSAID once daily for 7-14 days, short term use (1 day in the cat and 3 days in the dog) of atropine drops to help control ocular discomfort and a protective collar. The canine patient (Kelly) also underwent distichiasis removal with ‘blend’ electrolysis (electrolysis/diathermy) under the same anesthetic and started life-long use of Optimmune 2x day that was later reduced to 1x day.
The author retains all intellectual property rights of this article, including the text and images. The content of the article and its parts may not be reproduced or reused without specific permission from the author.